
Introduction
Peripheral ulcerative keratitis (PUK) is an inflammatory condition characterized by juxta-limbal epithelial defects and crescent-shaped corneal stromal thinning. The underlying inflammatory sources include both ocular and systemic infectious and noninfectious conditions.(1) More importantly, PUK may be the initial presenting sign of life-threatening systemic disease. There is an estimated incidence of 0.2 to 3 per million population per year(2) with no strong evidence to associate the keratitis with a specific age of onset, race, or ethnicity. Presenting symptomatology for PUK can vary and includes ocular pain, injection, foreign body sensation, photophobia, tearing, and decreased vision.(3) Urgent intervention is necessary to prevent corneal perforation from extreme thinning and treat the potentially fatal underlying cause. We present a case of PUK with multiple underlying etiologies that could serve as the inflammatory cause for disease.
Case report
A male in his 30s with no significant medical history presents with two years of eye irritation that has worsened over the past two months. The patient has been using tobramycin-dexamethasone drops without improvement. Best corrected visual acuity was 20/20 OU with normal intraocular pressures and reactive pupils.
Corneal examination was significant for a 4.5x1mm curvilinear epithelial defect in the inferior peripheral cornea with about 50% thinning of the corneal stroma. The conjunctiva adjacent to the area of cornea thinning was edematous and deeply injected. Given the concern for PUK versus an infectious sclerokeratitis, an infectious and autoimmune workup was obtained.
The patient was started on oral naproxen, moxifloxacin drops, prednisolone acetate drops, and erythromycin ointment. The patient later endorsed a travel history to Algeria once a year. The patient’s systemic work up was significant for a positive QuantiFERON gold and therefore the patient was started on a four-month course of rifampin by the RUSH Infectious Disease Department due to concern for latent tuberculosis (TB). While on this treatment, the keratitis, as well as the patient’s symptoms, began to improve.
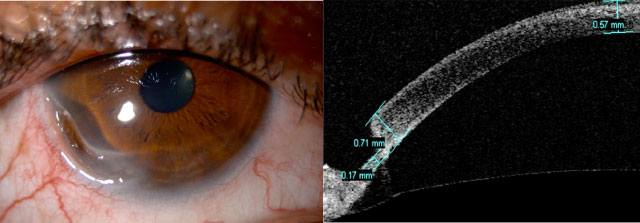
The patient was lost to follow-up for five months and returned with increasing eye pain. Rifampin therapy had been completed at that time and the patient remained on topical prednisolone acetate drops and oral naproxen. The curvilinear epithelial defect and stromal thinning had worsened (Figure 1a).
Anterior-segment OCT showed 76% thinning of the peripheral cornea with only 170 microns of corneal tissue remaining at its thinnest area. (Figure 1b).
Given the worsening corneal thinning, repeat autoimmune and infectious labs were obtained and patient was started on oral prednisone. Repeat workup was significant for a mildly positive pANCA. The patient was referred to Rheumatology for a vasculitis workup. The rheumatology evaluation was unremarkable and the patient’s epithelial defect continued to worsen on oral prednisone. The decision was made to take the patient to the operating room for a conjunctival resection with placement of amniotic membrane graft. The patient was admitted to the hospital for IV methyl prednisone prior to the procedure. The amniotic membrane graft was placed over the 9x6 mm epithelial defect and over the resected conjunctiva.
The patient remained on oral prednisone postoperatively. The cornea remained thin and superficial corneal neovascularization began to form within the thinned cornea. The conjunctival biopsy showed actinic degeneration but was otherwise unremarkable. After discussion with Rheumatology, the decision was made to transition the patient from oral prednisone to methotrexate. The patient’s epithelial defect and corneal thinning began to improve on this treatment. However, the underlying inflammatory etiology for the peripheral ulcerative keratitis remains undetermined.
Discussion
While the exact mechanism of PUK is unknown, the environment of the peripheral corneal may contribute to this inflammatory condition. Unlike the central cornea, the peripheral cornea has less neural innovation (4) and has direct blood supply that extends 0.5mm onto the cornea from the perilimbal capillaries.(5) This blood supply may directly bring inflammatory markers to the peripheral cornea. Other proposed mechanisms of PUK involve an imbalance of corneal collagenases and the collagenase inhibitors that maintain corneal integrity. Imbalances between the levels of matrix metalloproteinase (MMP) and tissue-inhibitors of MMP have been postulated as a mechanism of PUK.(6) Furthermore, elevated MMP-1 is correlated with corneal perforation in PUK.(7) These anatomical and pathophysiological factors are likely to contribute to the hallmark epithelial defects and peripheral stromal thinning of PUK.
The inflammatory etiology for PUK is vast, but is most commonly associated with rheumatoid arthritis, which is present in more than 34% of cases.(8) Other associated systemic inflammatory conditions include polyarteritis nodosa, inflammatory bowel disease, systemic lupus erythematosus, and granulomatosis with polyangiitis to name a few.(9) pANCA positivity is associated with granulomatosis with polyangiitis. One study demonstrated 3.1% of patients developing PUK have underlying granulomatosis with polyangiitis.(10) Other pANCA-associated vasculitis such as microscopic polyangiitis have also been associated with PUK.(11) Besides the ocular signs of possible systemic inflammation, this patient was otherwise asymptomatic. This highlights the difficulty in diagnosing ANCA-associated vasculitis and how ANCA positivity can be found in other systemic conditions and even be present when asymptomatic.(12,13)
Tuberculosis (TB)-induced PUK is well documented in the literature and is one of the infectious causes that should always be suspected.(14,15) Mycobacterium tuberculosis is an acid-fast-staining bacteria that can cause an inflammatory reaction in any part of the eye. In the United States, there are up to 13 million people living with latent TB.(16) In our case, the patient travels annually to Algeria which is a country with a higher incidence rate of TB than the United States.(17) This may have increased the patient’s risk of exposure to TB. Nevertheless, despite receiving the appropriate treatment for latent TB, the epithelial defect continued to progress. This implies that latent TB might not have been the underlying etiology for our patient’s PUK.
The main treatment goals for PUK are to support the cornea, prevent corneal superinfections, and assess for underlying systemic inflammatory and infectious causes. Topical steroids and antibiotics along with aggressive lubrication are implemented early in the treatment course. However, the mainstay of treatment for PUK is systemic corticosteroids or immunomodulation with the goal of decreasing systemic and ocular inflammation.(5) Transitioning from oral to intravenous steroids can prevent complications in vision threatening PUK.(3)
In cases that are severe or refractory to immunosuppressive treatment, surgical management is warranted. Ideally, surgery should be delayed until adequate immunosuppression is achieved to prevent recurrence.(18) Conjunctival resection adjacent to the area of juxta-limbal stromal thinning has shown to improve corneal healing by removing the inflammatory mediators.(19-22) This surgical procedure along with transitioning the patient to methotrexate helped to improve the epithelial defect and stromal thinning in our patient. Even with signs of improvement, close follow-up is needed as patients remain at risk for corneal perforation from recurrent inflammation if they have inadequate immunosuppression or poor compliance to treatment.(23)
References
- Gupta, Y., Kishore, A., Kumari, P., Balakrishnan, N., Lomi, N., Gupta, N., ... & Tandon, R. (2021). Peripheral ulcerative keratitis. Survey of Ophthalmology, 66(6), 977-998.
- Timlin, H. M., Hall, H. N., Foot, B., & Koay, P. (2018). Corneal perforation from peripheral ulcerative keratopathy in patients with rheumatoid arthritis: epidemiological findings of the British Ophthalmological Surveillance Unit. British Journal of Ophthalmology, 102(9), 1298-1302.
- Galor, A., & Thorne, J. E. (2007). Scleritis and peripheral ulcerative keratitis. Rheumatic Disease Clinics of North America, 33(4), 835-854.
- Müller, L. J., Vrensen, G. F., Pels, L., Cardozo, B. N., & Willekens, B. (1997). Architecture of human corneal nerves. Investigative ophthalmology & visual science, 38(5), 985-994.
- Yagci, A. (2012). Update on peripheral ulcerative keratitis. Clinical Ophthalmology (Auckland, NZ), 6, 747.
- Riley, G. P., Harrall, R. L., Watson, P. G., Cawston, T. E., & Hazleman, B. L. (1995). Collagenase (MMP-1) and TIMP-1 in destructive corneal disease associated with rheumatoid arthritis. Eye, 9(6), 703-718.
- Cao, Y., Zhang, W., Wu, J., Zhang, H., & Zhou, H. (2017). Peripheral ulcerative keratitis associated with autoimmune disease: pathogenesis and treatment. Journal of ophthalmology, 2017.
- Tauber, J., de la Maza, M. S., Hoang-Xuan, T., & Foster, C. S. (1990). An analysis of therapeutic decision making regarding immunosuppressive chemotherapy for peripheral ulcerative keratitis. Cornea, 9(1), 66-73.
- Messmer, E. M., & Foster, C. S. (1999). Vasculitic peripheral ulcerative keratitis. Survey of ophthalmology, 43(5), 379-396.
- Ismailova, D. S., Abramova, J. V., Novikov, P. I., & Grusha, Y. O. (2018). Clinical features of different orbital manifestations of granulomatosis with polyangiitis. Graefe's Archive for Clinical and Experimental Ophthalmology, 256(9), 1751-1756.
- Díaz-Valle, D., Benito-Pascual, B., Méndez-Fernández, R., Arriola-Villalobos, P., Arcos-Villegas, G., Molero-Senosiain, M., & Velo-Plaza, M. (2021). Peripheral ulcerative keratitis as presenting manifestation of systemic microscopic polyangiitis: a case report. Arquivos Brasileiros de Oftalmologia, 85, 82-84.
- Luqmani, R. A., Suppiah, R., Grayson, P. C., Merkel, P. A., & Watts, R. (2011). Nomenclature and classification of vasculitis–update on the ACR/EULAR diagnosis and classification of vasculitis study (DCVAS). Clinical & Experimental Immunology, 164(Supplement_1), 11-13.
- Jennette, J. C., Falk, R. J., & Wilkman, A. S. (1995). Anti-neutrophil cytoplasmic autoantibodies--a serologic marker for vasculitides. Annals of the Academy of Medicine, Singapore, 24(2), 248-253.
- Gupta, N., Chawla, B., Venkatesh, P., & Tandon, R. (2008). Necrotizing scleritis and peripheral ulcerative keratitis in a case of Sweet's syndrome found culture-positive for Mycobacterium tuberculosis. Annals of Tropical Medicine & Parasitology, 102(6), 557-560.
- Arora, T., Sharma, N., Shashni, A., & Titiyal, J. S. (2015). Peripheral ulcerative keratitis associated with chronic malabsorption syndrome and miliary tuberculosis in a child. Oman Journal of Ophthalmology, 8(3), 205.
- Division of Tuberculosis Elimination, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention. Data & Statistics | TB | CDC. Centers for Disease Control and Prevention. Published November 29, 2022. Accessed January 4, 2023. https://www.cdc.gov/tb-data/
- The World Bank Group. Incidence of tuberculosis (per 100,000 people) | Data. World Bank Open Data | Data. Accessed January 4, 2023. https://data.worldbank.org/indicator/SH.TBS.INCD
- Nobe, J. R., Moura, B. T., Robin, J. B., & Smith, R. E. (1990). Results of penetrating keratoplasty for the treatment of corneal perforations. Archives of Ophthalmology, 108(7), 939-941.
- Gris, O., Plazas, A., Lerma, E., Güell, J. L., Pelegrín, L., & Elíes, D. (2010). Conjunctival resection with and without amniotic membrane graft for the treatment of superior limbic keratoconjunctivitis. Cornea, 29(9), 1025-1030.
- Erikitola, O. O. C., Jawaheer, L., Ramaesh, K., & Anijeet, D. (2016). Conjunctival resection for peripheral ulcerative keratitis (PUK). Investigative Ophthalmology & Visual Science, 57(12), 1261-1261.
- Brown, S. I., & Mondino, B. J. (1984). Therapy of Mooren's ulcer. American journal of ophthalmology, 98(1), 1-6.
- Kalogeropoulos, C. D., Malamou–Mitsi, V. D., Aspiotis, M. B., & Psilas, K. G. (2004). Bilateral Mooren's ulcer in six patients: diagnosis, surgery and histopathology. International Ophthalmology, 25(1), 1-8.
- Ogra, S., Sims, J. L., McGhee, C. N., & Niederer, R. L. (2020). Ocular complications and mortality in peripheral ulcerative keratitis and necrotising scleritis: the role of systemic immunosuppression. Clinical & Experimental Ophthalmology, 48(4), 434-441.
